Vital signs
Vital signs
Vital signs:
- Temperature
- Pulse
- Respirations
- Blood pressure
- Oxygen saturation
Vital Signs
- Taken at each visit and compared to baseline
- Because of the importance of these measurements they are referred to as Vital Signs. they are important indicators of the body’s response to physical, environmental, and psychological stressors.
1.Body Temperature
- Core temperature – temperature of the body tissues, is controlled by the hypothalamus (control center in the brain) – maintained within a narrow range.
- Skin temperature rises & falls in response to environmental conditions & depends on blood flow to skin & amount of heat lost to external environment
- The body’s tissues & cells function best between the range from 36 deg C to 38 deg C
- Temperature is lowest in the morning, highest during the evening.
Temperature ( con't. )

Normal values of body temperature

Thermometers – 3 types
- Glass mercury – mercury expands or contracts in response to heat.
- Electronic – heat sensitive probe, (reads in seconds) there is a probe for oral/axillary use (red) & a probe for rectal use (blue).
- Infrared Tympanic (Ear) – sensor probe shaped like an otoscope in external opening of ear canal.

Fever (pyrexia)
It is the elevation of the body temperature above 37.5C, and is associated with an increased metabolic rate oxygen consumption and carbon dioxide production which cause a compensatory increase in heart rate and respiratory rate
so
It is contraindicated to perform exercises in case of fever.
2. Pulse Rate ( Heart Rate)
- Left ventricle contracts causing a wave of blood to surge through arteries – called a pulse. Felt by palpating artery lightly against underlying bone or muscle.
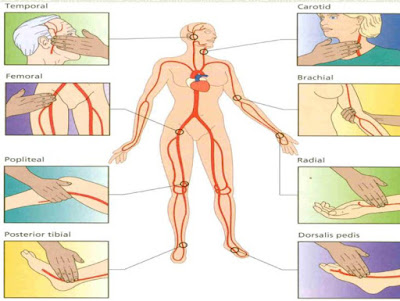
- Carotid, brachial, radial, femoral, popliteal, posterior tibial, dorsalis pedis.
- Assess: rate, rhythm, strength – can assess by using palpation & auscultation.
- Pulse deficit – the difference between the radial pulse and the apical pulse – indicates a decrease in peripheral perfusion from some heart conditions.
Procedure for Assessing Pulses
- Peripheral – place 2nd, 3rd & 4th fingers lightly on skin where an artery passes over an underlying bone. Do not use your thumb (feel pulsations of your own radial artery). Count 30 seconds X 2, if irregular – count radial for 1 min. and then apically for full minute.
- Apical – beat of the heart at it’s apex or PMI (point of maximum impulse) – 5th intercostal space, midclavicular line, just below lt. nipple – listen for a full minute “Lub-Dub”
- Lub – close of atrioventricular (AV) valves – tricuspid & mitral valves
- Dub – close of semilunar valves – aortic & pulmonic valves
Assess: rate, rhythm, strength & tension
- Rate – N – 60-100, average 80 bpm
- Tachycardia – greater than 100 bpm
- Bradycardia – less than 60 bpm
- Rhythm – the pattern of the beats (regular or irregular)
- Strength or size – or amplitude, the volume of blood pushed against the wall of an artery during the ventricular contraction
- weak (lacks fullness)
- Full, bounding (volume higher than normal)
- Absent (cannot be felt or heard)
0----------------- 1+ -----------------2+----------------- 4+
Absent weak Normal Bounding
Normal Heart Rate
Age | Heart Rate |
| Infants (1 m - 2 y ) | 120-160 |
| School ages ( 6 y - 11 y ) | 75-100 |
| Adult | 60-100 |

Radial
The radial pulse is felt on the wrist , just under the thumb

Brachial
Cubital fossa, medial to biceps tendon.

Carotid
Just lateral to upper border of thyroid cartilage medial to SCM.
Carotid artery can’t be assessed from standing to avoid fainting and the assessment must be done unilateral.
Carotid artery can’t be assessed from standing to avoid fainting and the assessment must be done unilateral.

Femoral Artery
Below inguinal ligament, midway between ASIS and pubic symphysis

Popliteal
Flex knee before palpating.
In midline, on popliteal side of lower end of femur (the most difficult to palpate )
*It can be assessed from prone position with flexed knee ( but not for pregnancy , obese and old age )

Posterior tibial
Posterior, inferior to medial malleolus, between flexor digitorum longus and flexor hallucis longus

Dorsalis pedis
Lateral to extensor halluces longus, over tarsal bones
Measure HR by stethoscope

beat of the heart at it’s apex or PMI (point of maximum impulse) – 5th intercostal space, midclavicular line, just below the nipple – listen for a full minute “Lub-Dub”
3.Respiratory Rate
- Assess by observing Rate, Rhythm & Depth
- Inspiration – inhalation (breathing in)
- Expiration – exhalation (breathing out)
- I&E is automatic & controlled by the medulla oblongata (respiratory center of brain)
- Normal breathing is active & passive
- Asses after taking pulse, while still holding hand, so patient is unaware you are counting respiration

The normal values of respiratory rate are approximately
- 12-20 breaths/min for normal adult.
- 30-60 breaths/min for normal new born.
- 25-35 breaths/min for 1 year old.
- 20-25 breaths/min for preschool child.

